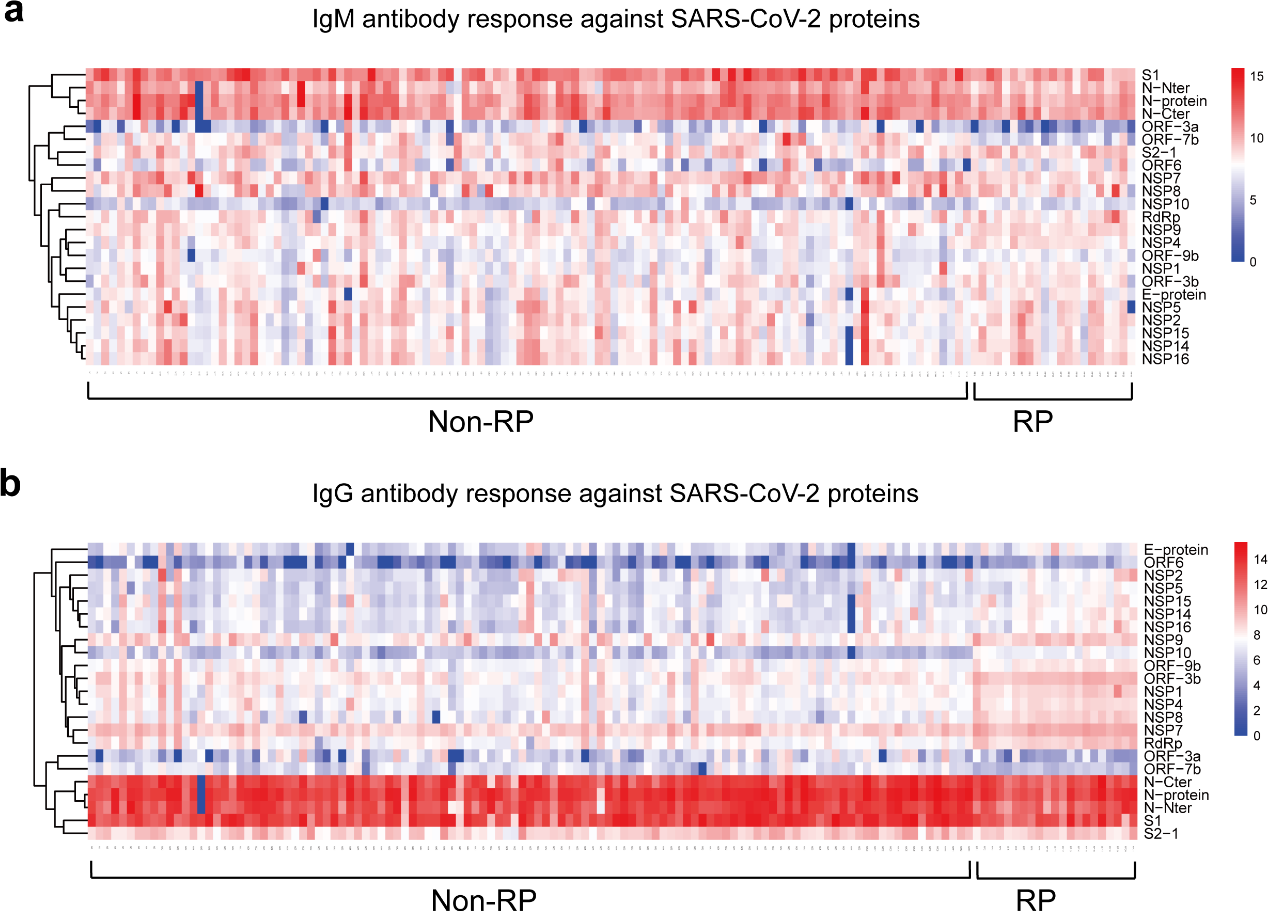
Impaired humoral immunity of COVID-19 patients with re-detectable positive RNA test after recoveryQing Lei1,2, Caizheng Yu3, Yang Li4, Hongyan Hou5, Banga Ndzouboukou Jo-Lewis1, Zhuqing Ouyang1, Yandi Zhang1, Xiaosong Lin1, Zongjie Yao1, Fu hui1, Ziyong Sun5, Feng Wang5,*, Shengce Tao4,*, Xionglin Fan1,*1Department of Pathogen Biology, School of Basic Medicine, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, China.2Department of Medical Laboratory, The Central Hospital of Wuhan, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, China.3Department of Public Health, Tongji Hospital, Tongji Medical College, Huazhong University ofScience and Technology, Wuhan, China.4Shanghai Center for Systems Biomedicine, Key Laboratory of Systems Biomedicine (Ministry of Education), Shanghai Jiao Tong University, Shanghai 200240, China5Department of Laboratory Medicine, Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, China.*Correspondence’ e-mail: Xiong-lin Fan([email protected]), Sheng-ce Tao([email protected]), Feng Wang([email protected])To the Editor,The coronavirus disease 2019 (COVID-19), caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), has rapidly spread worldwide.1,2As of May 28, 2020, WHO estimated that there had been 169 million confirmed cases and 3.5 million patients died from SARS-CoV-2 infection.3 Due to lack of etiological treatments, about 3.5%-18% of discharged COVID-19 patients after recovery had a re-tested positive result for SARS-CoV-2 RNA, who was also named after re-detectable positive patients (RP).4-8 Moreover, RP patients may have the potential for virus transmission.9,10However, the mechanism of the occurrence of RP patients remains little known.Humoral immunity, especially neutralizing antibody plays an important role in preventing against SARS-CoV-2 infection, and even disease progression. To elucidate the role of humoral immunity in RP patients, we compared anti-SARS-CoV-2 IgM and IgG antibody responses between RP and non-RP patients in this study. 21 RP patients from Wuhan Pulmonary Hospital (Wuhan, China) between Jan 11, 2020, and April 1, 20204 and 113 non-RP patients discharged from Tongji Hospital, between February 17, 2020, and April 28, 2020 were recruited. Non-RP had negative NAT results while RP patients had at least once positive result during weekly follow-up after discharge. The median time from discharge to a positive retest of 21 RP patients was 14 (range: 4-24) days, and their serum samples were collected at the time of the positive retest. Besides, the serum samples of 113 non-RP patients were collected on the 14th day after discharge. At the same time, we collected serum samples of 601 non-COVID-19 controls including healthy donors, lung cancer patients, patients with autoimmune diseases from Ruijin Hospital (Shanghai, China), Tongren Hospital (Shanghai, China), or National Institutes for Food and Drug Control.11 All serum samples were stored under -80oC until use.First, we used a homemade proteome microarray to detect serum IgM (red) or IgG (green) antibody responses against 20 out of 28 predicted proteins of SARS-CoV-2 with Alexa Fluor 647-conjugated donkey anti-human IgM and Cy3-conjugated goat anti-human IgG (Figure S1) , as previously described. Based on the fluorescent intensity extracted from the microarray, anti-SARS-CoV-2 IgM and IgG profiles for each serum sample were established (Figure 1 ). Interestingly, there were differential IgM and IgG profiles observed between RP patients and non-RP patients. RP patients elicited lower levels of IgM and IgG responses against NSP7, ORF3a, and ORF7b, as well as anti-S1 and N specific IgM and IgG than non-RP patients (Figure 2 ). More importantly, RP patients induced higher levels of specific IgG antibodies against most non-structural and accessory proteins, such as NSP1, NSP2, NSP4, NSP5, NSP7, NSP8, NSP9, NSP10, RdRp, NSP14, NSP15, NSP16, ORF-3b, ORF6, and ORF9b, and E structural protein (Figure 2 ). Previously, the levels of IgG responses to NSP4, NSP7, NSP9, NSP10, RdRp, NSP14 and ORF3 might be related with the poor prognosis and severity of COVID-19.Further, a pseudotyped virus-based neutralization assay platform was used to detect the levels of serum nAb. Unexpectedly, RP patients elicited lower levels of nAb than non-RP. In particular, 90.5% (19/21) RP patients could not detect the nAb response (NT50<10) (Figure S2 ).In conclusion, RP patients impaired humoral immunity, which might benefit the replication of residual SARS-CoV-2 virus in vivo. Our findings have an important impact on improving clinical management. The criterion for patients’ recovery and discharge should be improved to prevent recurrence , such as serological detection and even nAb response, besides persisting and repeated NAT screening.