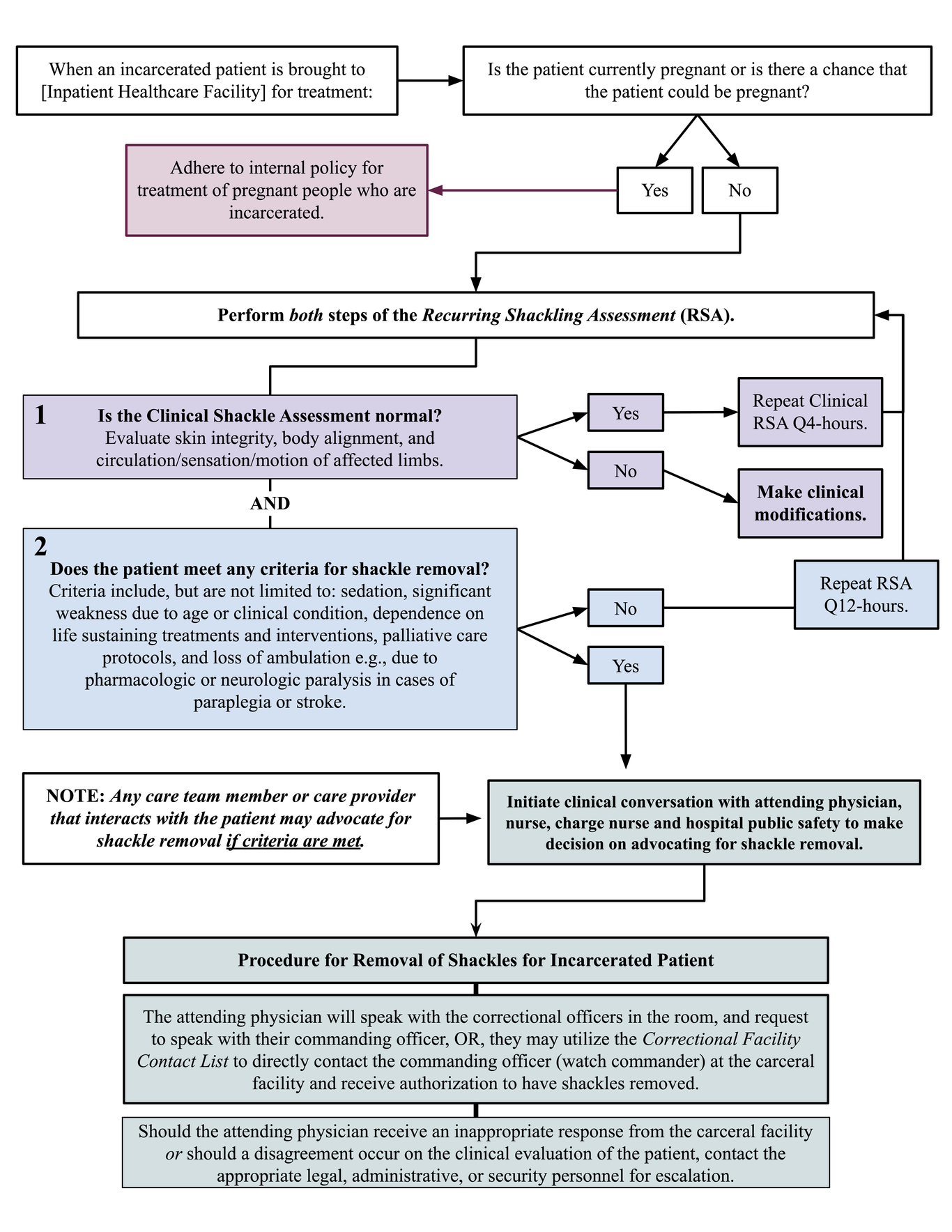
AbstractMedical students (NSB, NM, JDW), spearheaded revision of the written policy and clinical practice for shackling incarcerated patients at Boston Medical Center, the largest safety net hospital in New England. Across hospitals in the United States, routine shackling of incarcerated patients with metal handcuffs is widespread, except for pregnant prisoners, regardless of consciousness, immobility, illness severity, or age. The modified policy includes individualized assessment and allows incarcerated patients to be unshackled if they meet defined criteria. The students also formed the Stop Shackling Patients Coalition (SSP Coalition) of clinicians, public health practitioners, human rights advocates, and community members who share the goal of humanizing the inpatient treatment of incarcerated patients.IntroductionRoutine shackling of incarcerated patients with metal handcuffs is widespread in hospitals across the United States (US), with the exception of pregnant prisoners. Despite harmful effects on patients and national attention to health equity, incarcerated patients are routinely shackled regardless of consciousness, immobility, illness severity, or age.1,2 A large cohort study (n = 1078) of Israeli hospitals found that 84% of incarcerated patients who have severely impaired mobility for medical reasons are shackled, nonetheless.3 The discriminatory and dehumanizing practice of routinely applying shackles to incarcerated patients exacerbates existing care disparities by violating both medical ethics and human rights principles. The 2018 federal First Step Act prohibited “the shackling of pregnant prisoners in federal custody, except in certain cases.”4 As the name of this criminal justice bill suggests, the ban did not entirely eliminate shackling and the practice continues to impact nonpregnant incarcerated patients.5There is a common misconception amongst healthcare professionals that they cannot influence the use of shackles to restrain their patients. By not challenging this practice within our healthcare institutions, the correctional system essentially governs aspects of patient care. Protocols for shackling incarcerated patients can and must be changed to respect human dignity and health, while simultaneously providing safety in the workplace.6-9Harms to IndividualsShackling impacts physical health in several ways. In the hospital setting, restraints can result in skin breakdown, circulation compromise, compressive neuropathies, fractures, increased fall risk, increased risk of delirium, and predisposition to severe vascular injury.6,8,10,11 Clinicians may be limited in their ability to perform a thorough physical examination.8Clinician bias against the shackled patient may also harm the clinician-patient relationship. In fact, the presence of shackles negatively affects empathy, precipitates diagnostic skepticism and elicits unsubstantiated fears of personal harm by the patient.6 Shackles have led to insensitive, inappropriate, neglectful, or abusive actions by staff or associated authority figures, which in turn evokes a response of fear in patients along with a loss of trust in the care team.12 These negative healthcare interactions further stress incarcerated patients’ post-carceral challenges within the healthcare system.13Human Rights ViolationsRoutine shackling of incarcerated patients violates foundational international human rights principles, including those contained in the Universal Declaration of Human Rights, the International Convention on the Elimination of All Forms of Racial Discrimination, and the International Covenant on Civil and Political Rights.14-16 These principles are designed to protect human dignity and protect persons from discrimination and cruel, inhuman, and degrading treatment. Shackling patients who are critically ill or at the end of life is an affront to their human dignity, and increases pain and suffering in this vulnerable time. Routine shackling violates the United Nations (UN) Standard Minimum Rules for the Treatment of Prisoners (The Nelson Mandela Rules) – the internationally accepted standard for the treatment of prisoners.17 Rule 48 addresses the use of restraints. See Box 1. Box 1: UN Standard Minimum Rules (The Nelson Mandela Rules) Rule 48 When the imposition of instruments of restraint is authorized in accordance with paragraph 2 of rule 47, the following principles shall apply: (a) Instruments of restraint are to be imposed only when no lesser form of control would be effective to address the risks posed by unrestricted movement; (b) (c) The method of restraint shall be the least intrusive method that is necessary and reasonably available to control the prisoner’s movement, based on the level and nature of the risks posed; Instruments of restraint shall be imposed only for the time period required, and they are to be removed as soon as possible after the risks posed by unrestricted movement are no longer present. Instruments of restraint shall never be used on women during labor, during childbirth and immediately after childbirth. In accordance with these Mandela Rules and the Charter of Fundamental Rights of the European Union, the head of the British prison service proclaimed that the “shackling of patients in hospital[s] should not occur,” emphasizing that “security is important, but it should never blind us to the overriding need for compassion and humanity.”18, 19 In the Netherlands, chains are never used and handcuffs are used only in exceptional circumstances.20 Our work amended shackling practices to introduce a risk-stratified, individualized protocol for American hospitals that aligns with human rights principles better upheld by Western nations. 21, 22From Changing Hospital Policy to Launching a National Movement We began by writing and circulating a petition to local hospital affiliates and community members to raise awareness and support.23 The petition then spread nationally, amassing 780 signatures across 129 institutions. The response demonstrated a consensus for change that enabled us to engage the hospital’s executive leadership in policy reform. Next, we solicited input from key hospital stakeholders including public safety and patient-facing staff such as nurses, as well as medical, nursing leadership, and legal hospital leadership. Identifying shared values for patient care helped generate feedback to balance concerns for safety and liability with human dignity. We then engaged with hospital administration and proposed a modification to existing hospital policy. Following multiple meetings with and input from key stakeholders, the policy on shackling incarcerated patients was officially modified in February 2023. The core of the modified policy is a process that allows for the removal or modification of shackling in certain incarcerated patients and provides hospital personnel with a detailed protocol for the assessment and implementation of this policy. The policy outlines a schema for communication and decision-making among carceral facilities, hospital security, and the patient’s healthcare team with the goal of providing dignified and humane care to incarcerated patients while maintaining hospital security. The discourse around shackling practices reached beyond the walls of our hospital, inciting a national discussion not only regarding the issue of shackling patients but how this practice could be brought to an end. In parallel to the conversations we were leading and progress we were making within Boston Medical Center, we also launched the Stop Shackling Patients Coalition (SSP) – a body of clinicians, public health practitioners, human rights advocates, and community members who share the goal of humanizing the inpatient treatment of incarcerated patients. SSP has now grown into a diverse task force and learning collaborative that meets to empower healthcare institutions from across the United States to change their shackling policies.