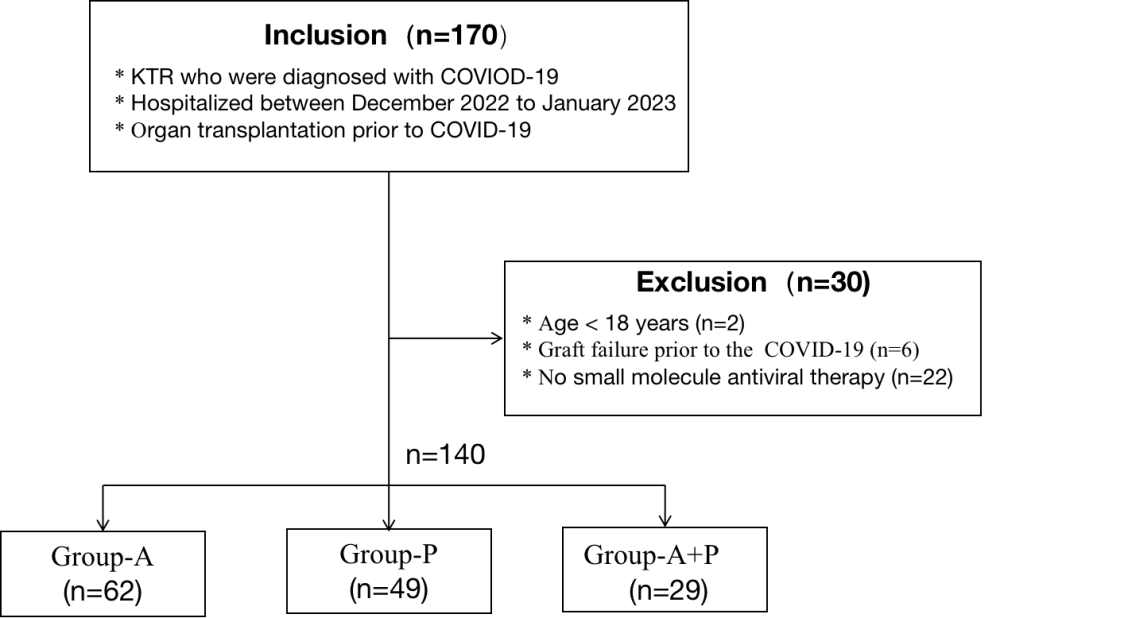
Background We analyzed the effects of small-molecule antiviral treatment for coronavirus disease-2019 (COVID-19) Omicron strain in kidney transplant recipients. Methods We enrolled 140 kidney transplant patients admitted for COVID-19-related pneumonia were treated using small-molecule antivirals. Patients were divided into three groups: azvudine (n=62), paxlovid (n=49), and a combination of azvudine+paxlovid (A+P, n=29). Differences in clinical outcomes owing to COVID-19 infections were compared among three groups. Results Paxlovid group had a higher proportion of comorbid diabetes than the other two groups (P=0.032). There were differences in the clinical typing of the coronavirus , with the highest proportion of heavy and critical cases in the A+P group (35.5%). The immunosuppression prior to infection did not differ among the groups; however, after adjusting for immunosuppression during antiviral treatment, differences were observed. Of the 140 patients, 125 (89.29%) had fever, 114 (81.43%) had cough, and 66 (47.1%) had malaise. Combination of two or more symptoms were found in 90% patients. Mean length of hospitalization was slightly longer in the combination group than in the azvudine and paxlovid groups. Four deaths, all in the A+P group; five cases of loss of function, two in the paxlovid group and three in the A+P group; and acute kidney injury occurred in 30 patients with 7 in the azvudine, 17 in paxlovid, and 6 in A+P groups. Conclusion The use of small-molecule medications may be the optimal treatment approach; however, they should be modified based on the patients’ conditions, such as clinical symptoms, laboratory results, paraclinicals, and examinations.