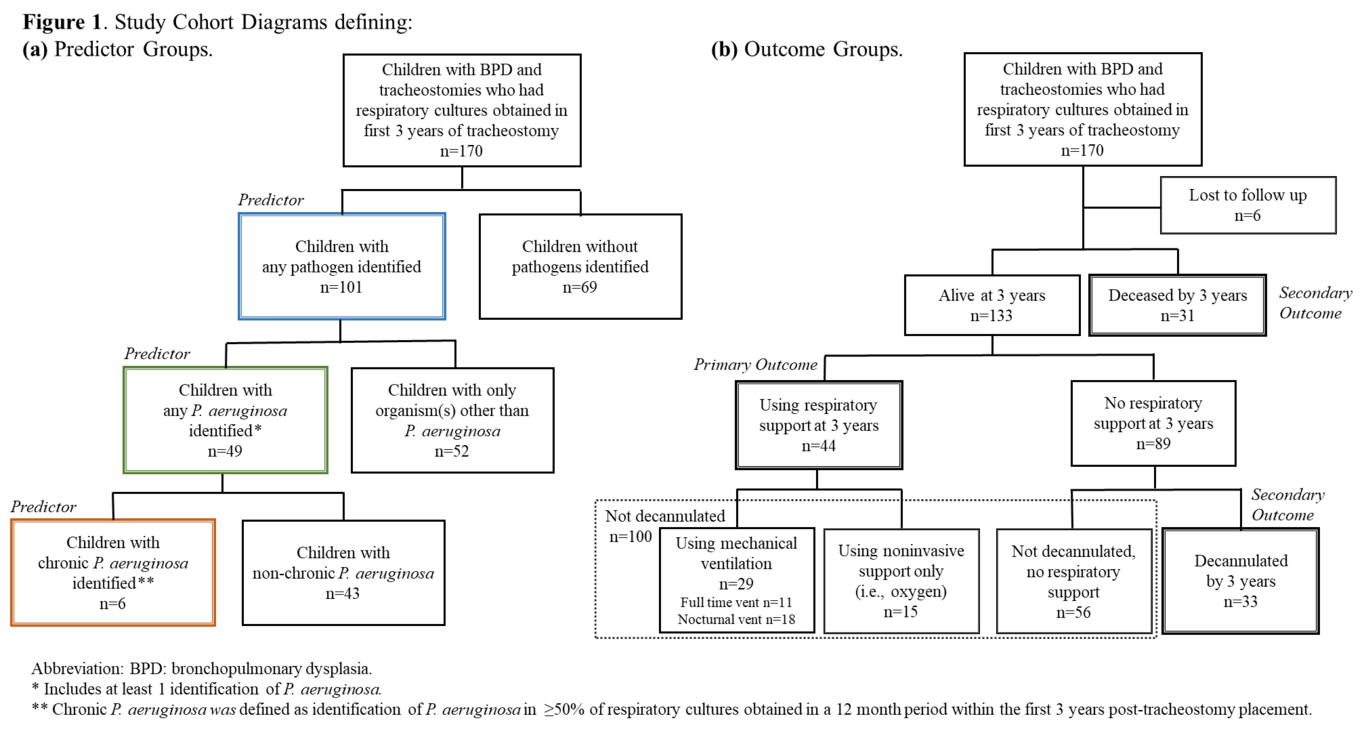
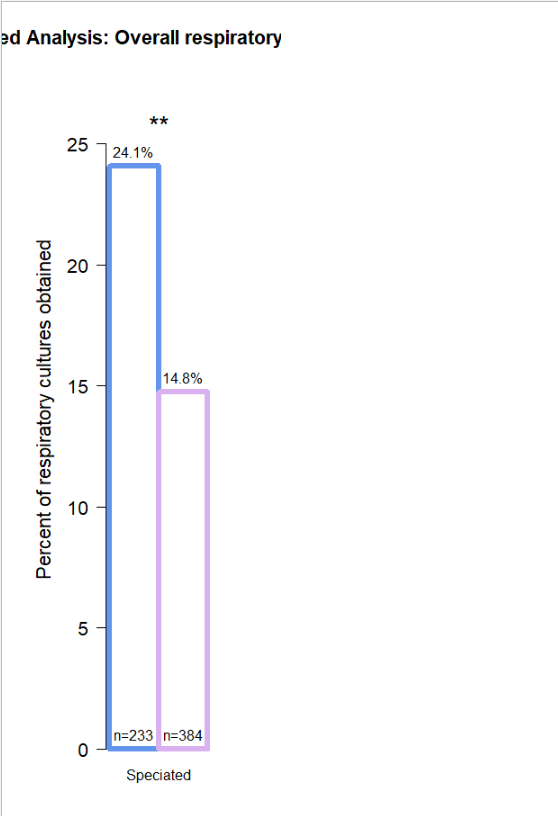
Background: While bacteria identification on respiratory cultures is associated with poor short-term outcomes in children with bronchopulmonary dysplasia (BPD) and tracheostomies, the influence on longer-term respiratory support needs remains unknown. Objective: To determine if respiratory culture growth of pathogenic organisms is associated with ongoing need for respiratory support, decannulation, and death at 3 years post-tracheostomy placement in children with BPD and tracheostomies. Methods: This single center, retrospective cohort study included infants and children with BPD and tracheostomies placed 2010-2018 and >1 respiratory culture obtained in 36 months post-tracheostomy. Primary predictor was any pathogen identified on respiratory culture. Additional predictors were any Pseudomonas aeruginosa and chronic P. aeruginosa identification. Outcomes included continued use of respiratory support (e.g., oxygen, positive pressure), decannulation, and death at 3 years post-tracheostomy. We used Poisson regression models to examine the relationship between respiratory organisms and outcomes, controlling for patient-level covariates and within-patient clustering. Results: Among 170 children, 59.4% had a pathogen identified, 28.8% ever had P. aeruginosa, and 3.5% had chronic P. aeruginosa. At 3 years, 33.1% of alive children required ongoing respiratory support and 24.8% achieved decannulation; 18.9% were deceased. In adjusted analysis, any pathogen and P. aeruginosa were not associated with ongoing respiratory support or mortality. However, P. aeruginosa was associated with decreased risk of decannulation (aRR 0.48, 95% CI 0.23-0.98). Chronic P. aeruginosa was associated with lower survival probability. Conclusion: Our findings suggest that respiratory pathogens including P. aeruginosa may not promote long-term respiratory dysfunction, but identification of P. aeruginosa may delay decannulation.