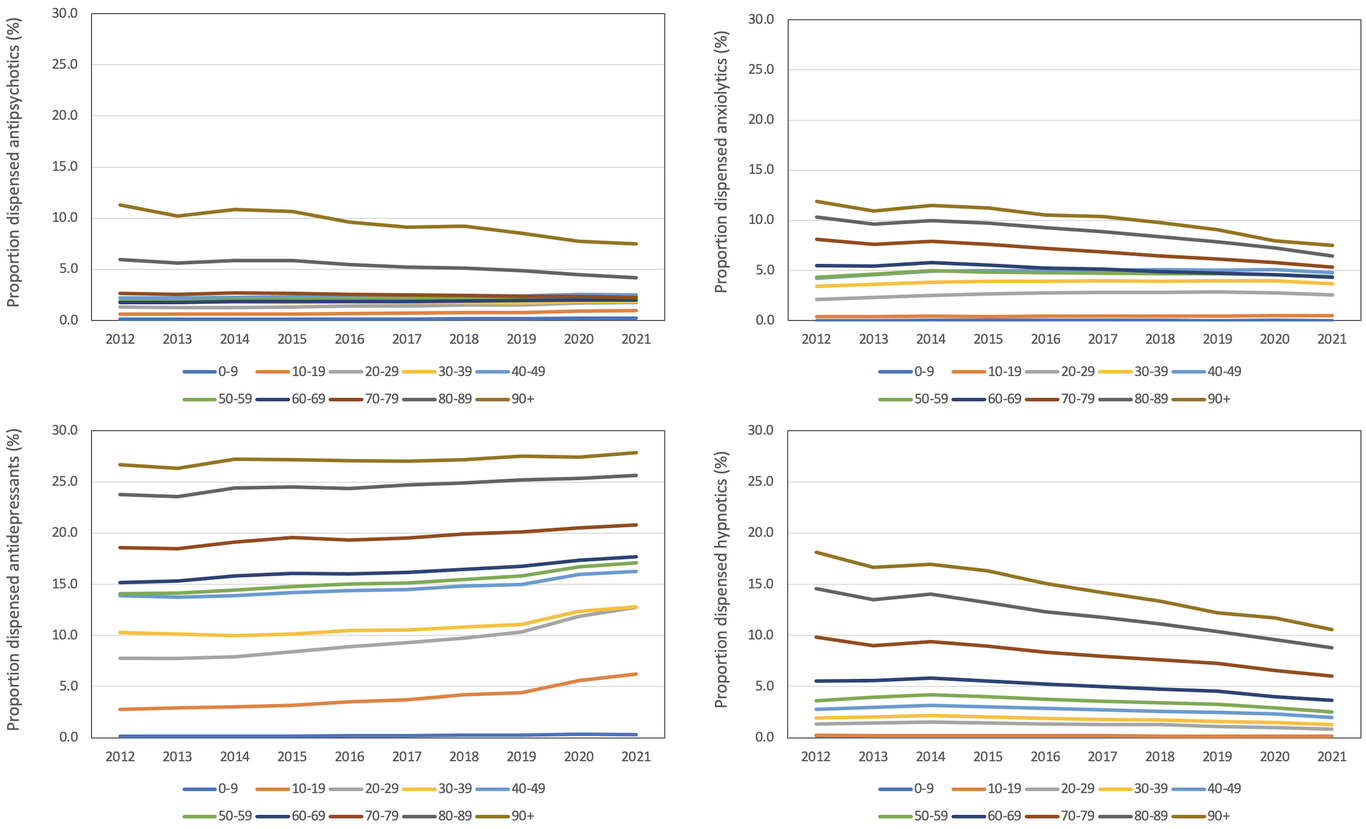
Purpose: To determine the proportion of Australians dispensed psychotropic medications between 2013 and 2022 according to their age. Methods: Services Australia provided a de-identified 10% random Pharmaceutical Benefits Scheme (PBS) sample that allowed us to determine the proportion of Australians dispensed at least one script per year for the use of antipsychotics, antidepressants, anxiolytics, and hypnotics. The classification of medications followed Anatomical Therapeutic Chemical (ATC) coding. Participants were stratified into 10-year age groups from 0-9 to ≥90 years, and sex was coded as male/female. We used logit models to analyse the data. Results: The number of records per year ranged from 1,540,520 to 1,746,402, and 54.10% were for females. A greater proportion of older adults, particularly those aged ≥70 years, were dispensed antipsychotics, antidepressants, anxiolytics, and hypnotics than any other age-group. The proportion of people dispensed antipsychotics, anxiolytics, and hypnotics declined between 2013 and 2022, but increased for antidepressants, most markedly for adolescents and young adults. Females were more frequently dispensed antidepressants, anxiolytics, and hypnotics than males, but males were more frequently dispensed antipsychotics than females. Conclusions: Older age groups and females are the most frequent recipients of psychotropic medications dispensed in Australia. The organisation and resourcing of health services should reflect this reality.