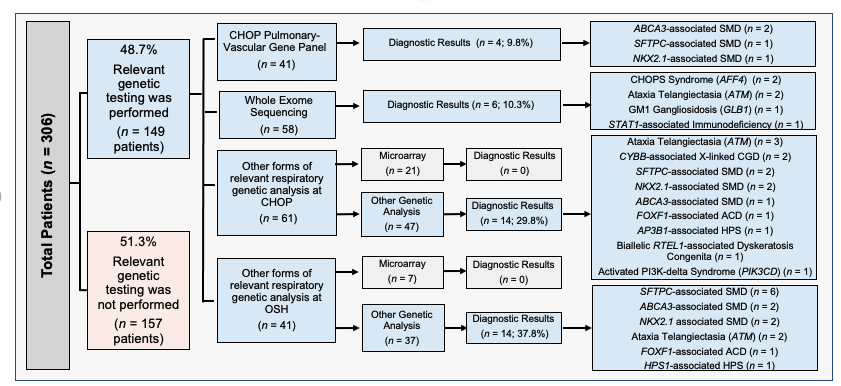
Childhood interstitial lung disease (chILD) is a heterogeneous group of diffuse lung diseases (DLD) that can be challenging to diagnose. With relative rarity of individual entities, data are limited on disease prevalence, care patterns, and healthcare utilization. The objective of this study was to evaluate chILD prevalence and review diagnostic and clinical care patterns at our center. A single-center, retrospective cohort study was conducted of patients receiving care at the Children’s Hospital of Philadelphia (CHOP) between January 1, 2019, and December 31, 2021. Through query of selected ICD-10 billing codes relevant for chILD/DLD, a total of 306 patients were identified receiving care during this period. Respiratory symptom onset was documented to have developed before two years of age for 40% of cases. The most common diagnostic categories included those with oncologic disease (21.2%), bronchiolitis obliterans (10.1%), and connective tissue disease (9.5%). Genetic testing was performed in 49% of cases, while 36% underwent lung biopsy. Hospitalization at CHOP had occurred for 80.4% of patients, with 45.1% ever hospitalized in an intensive care unit. One-third of children had required chronic supplemental oxygen. Seven (2.3%) patients died during this three-year period. Collectively, these data demonstrate the scope of chILD and extent of health care utilization at a large volume tertiary care center. This approach to cohort identification and EMR-driven data collection in chILD provides new opportunities for cohort analysis and will inform the feasibility of future studies.