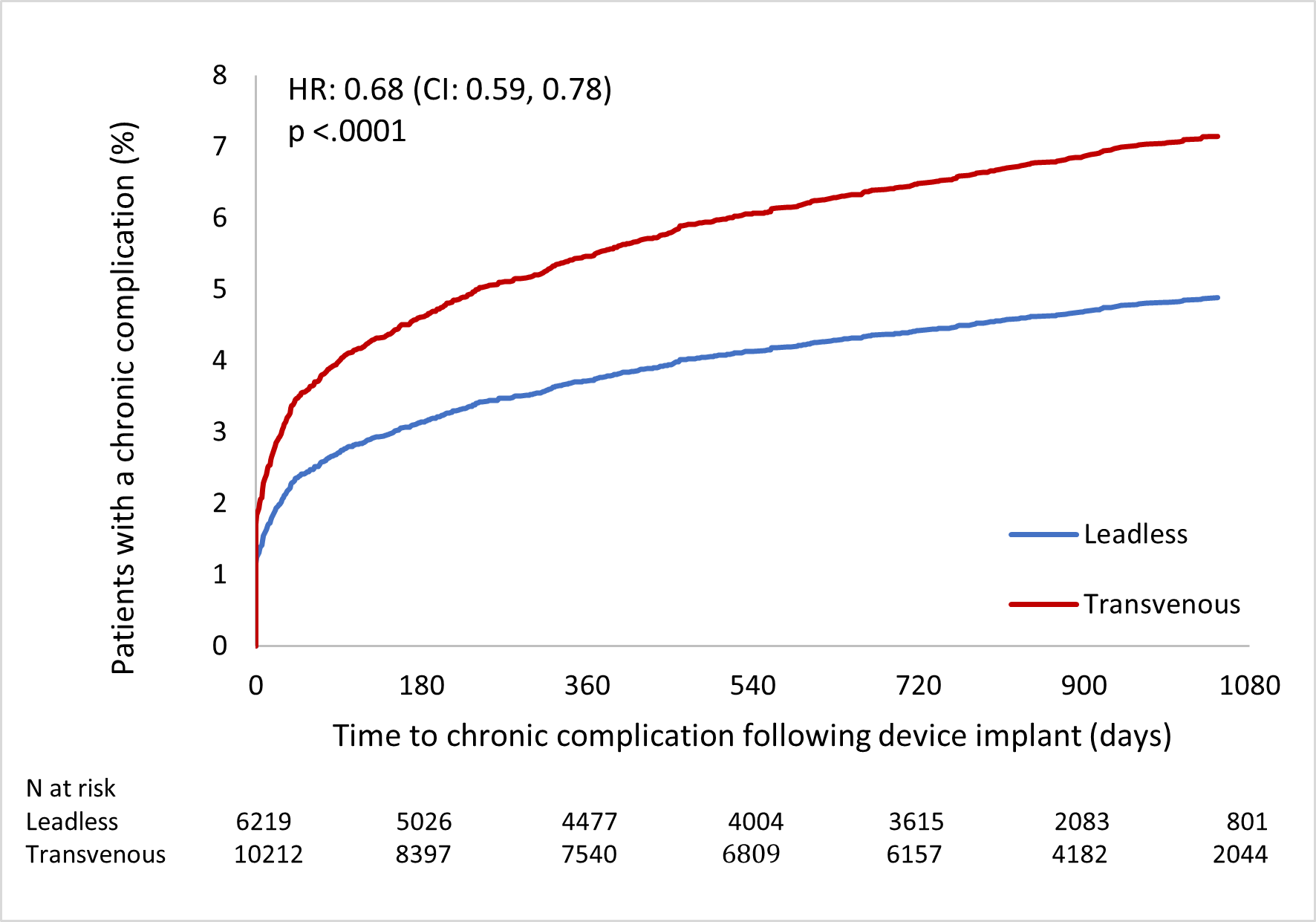
Background: The Micra Coverage with Evidence Development (CED) Study is a novel comparative analysis of Micra (leadless VVI) and transvenous single-chamber ventricular pacemakers (transvenous VVI) using administrative claims data. Objective: To compare chronic complications, device reinterventions, heart failure hospitalizations, and all-cause mortality after 3 years of follow-up. Methods: U.S. Medicare claims data linked to manufacturer device registration information were used to identify Medicare beneficiaries with a de novo implant of either a Micra VR leadless VVI or transvenous VVI pacemaker from March 9, 2017-December 31, 2018. Unadjusted and propensity score overlap-weight adjusted Fine-Gray competing risk models were used to compare outcomes at 3 years. Results: Leadless VVI patients (N=6,219) had a 32% lower rate of chronic complications and a 41% lower rate of reintervention compared with transvenous VVI patients (N=10,212) (chronic complication hazard ratio [HR] 0.68; 95% CI, 0.59-0.78; reintervention HR 0.59; 95% CI 0.44-0.78). Infections rates were significantly lower among patients with a leadless VVI (<0.2% versus 0.7%, P<0.0001). Patients with a leadless VVI also had slightly lower rates of heart failure hospitalization (HR 0.90; 95% CI 0.84-0.97). There was no difference in the adjusted 3-year all-cause mortality rate (HR 0.97; 95% CI, 0.92-1.03). Conclusion: This nationwide comparative evaluation of leadless VVI versus transvenous VVI de novo pacemaker implants demonstrated that the leadless group had significantly fewer complications, reinterventions, heart failure hospitalizations, and infections than the transvenous group at 3 years, confirming that the previously reported shorter-term advantages associated with leadless pacing persist and continue to accrue in the medium-to-long-term.