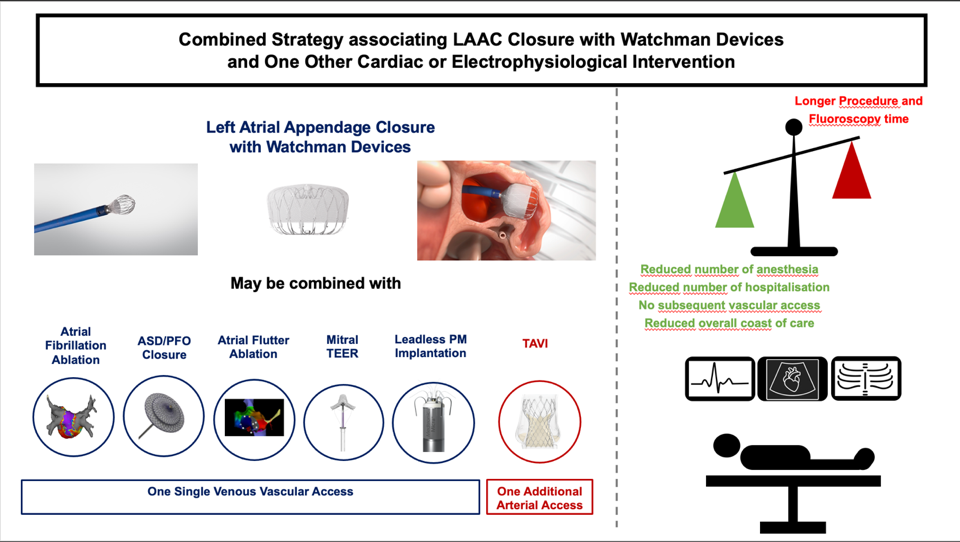
Introduction: Percutaneous left atrial appendage closure (LAAC) is an alternative to oral anticoagulant (OAC) in patients with non-valvular atrial fibrillation (AF) and contraindication to long-term OAC. Combined strategy with percutaneous LAAC at the same time of other cardiac structural or electrophysiological procedure has emerged as an alternative to staged strategy. Aim: To describe our experience of combined LAAC procedures using Watchman™ devices. Method: All patients with combined LAAC procedure using Watchman™ (WN) devices performed from 2016-2021 were included. The primary safety endpoint was a composite of periprocedural complications and adverse events during follow-up. The primary efficacy endpoint included strokes, systemic embolisms, major bleeding, and cardiovascular death. Results: Since 2016, among the 157 patients who underwent LAAC using WN devices, 16 underwent a combined strategy: 6 TEMVR (37%), 6 typical atrial flutter ablation (37%), 2 LP implantation (13%) and 2 atrial fibrillation ablation (13%). The WN device was successfully implanted in 98% and 100% for single and combined LAAC respectively (p = 0.63). Median follow-up was 13 months (IQR 25/75 3/24) in the whole cohort. Device related complications occurred in 6 out of 141 patients (4%) who underwent single LAAC and in no (0/16) patient in the combined LAAC procedure (p=ns). The procedural related complications did not differ significantly between groups (5% vs 12%, respectively in the single and combined group, p=0.1). Conclusion: Combined procedure combining LAAC using the Watchman™ devices and one other structural or electrophysiological procedure is safe and effective. Larger series are needed to confirm these results.