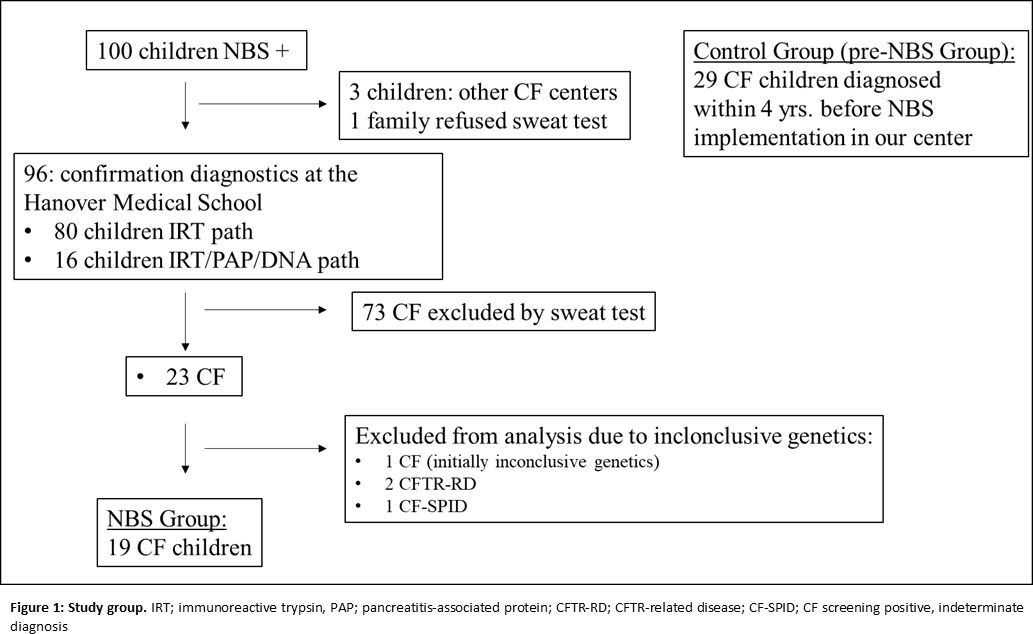
Background: Newborn screening (NBS) has been shown to improve CF disease course and has been widely implemented worldwide. This monocentric study compared children diagnosed by NBS vs. a cohort preceding the implementation of NBS in Germany in 2016 to evaluate ascribed benefits of NBS. Methods: We compared all children with confirmed CF diagnosis (n=19, “NBS group”) out of all children presenting with positive NBS at our center after implementation of NBS (n=100) to children diagnosed with CF at our center within 4 years before NBS implementation (n=29, “pre-NBS group”) for outcomes of anthropometry, gastrointestinal and pulmonary disease manifestations and respiratory microbiology. Results: Children diagnosed by NBS had a lower incidence of initial feeding problems (15% vs. 41%), had a higher BMI z-score at diagnosis and higher mean z-scores for BMI, weight and length during the study period. Children in the pre-NBS group displayed higher proportions of oxygen-dependent pulmonary exacerbations (10% vs. 0%), a significantly lower amount of normal bacterial flora (p=0.005) along with a significantly higher number of throat swab cultures positive for Pseudomonas aeruginosa (p=0.0154) in the first year of life. Yet, pulmonary imaging did not reveal less pulmonary morbidity in the NBS compared to the pre-NBS group. Conclusions: Our results confirm that NBS for CF leads to earlier diagnosis and improves nutritional outcomes in early childhood. Although trajectories of structural lung damage at early age were unaffected by NBS, NBS positive CF patients at preschool age displayed less severe pulmonary exacerbations and pathological bacteria in throat swabs.