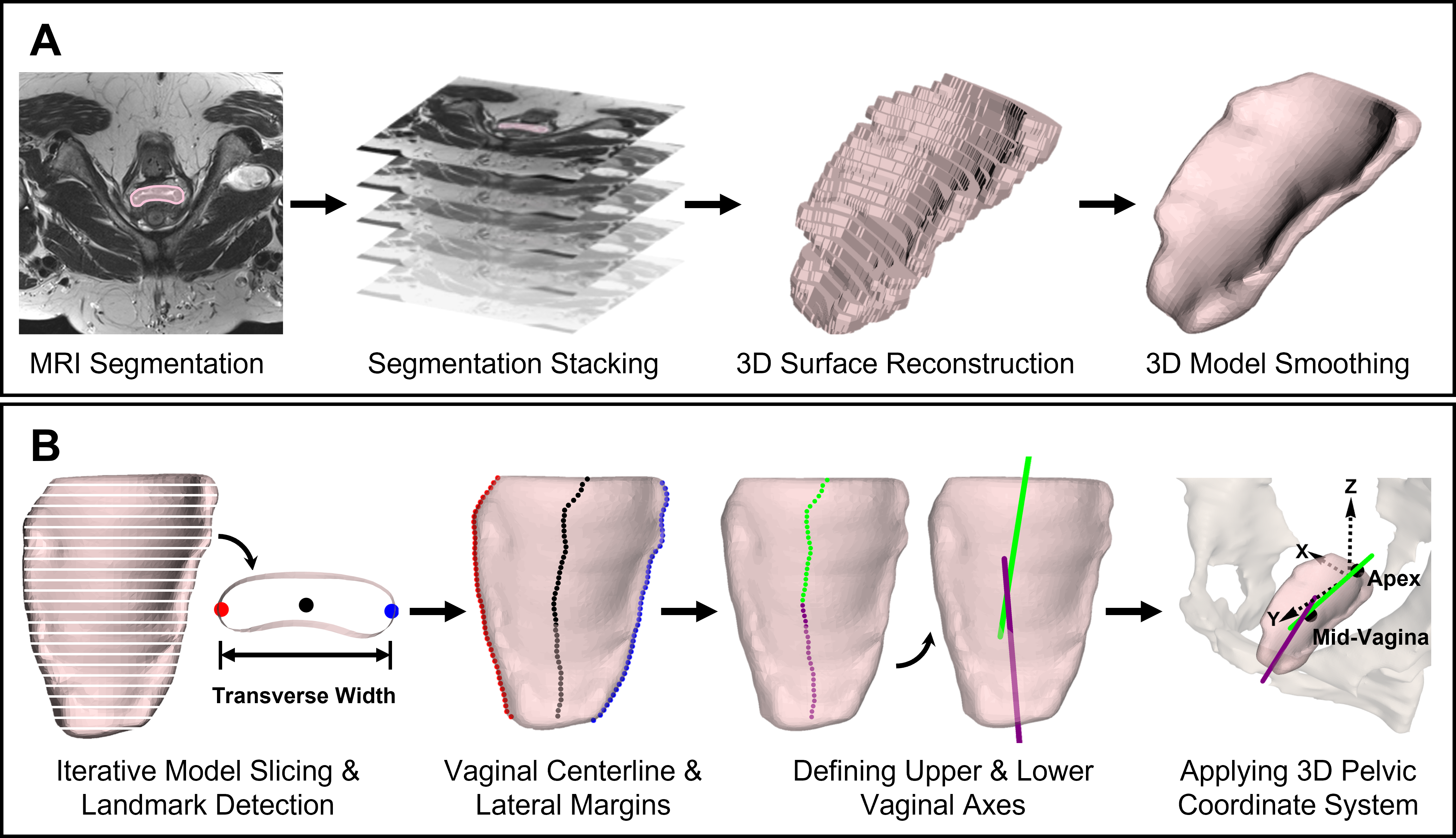
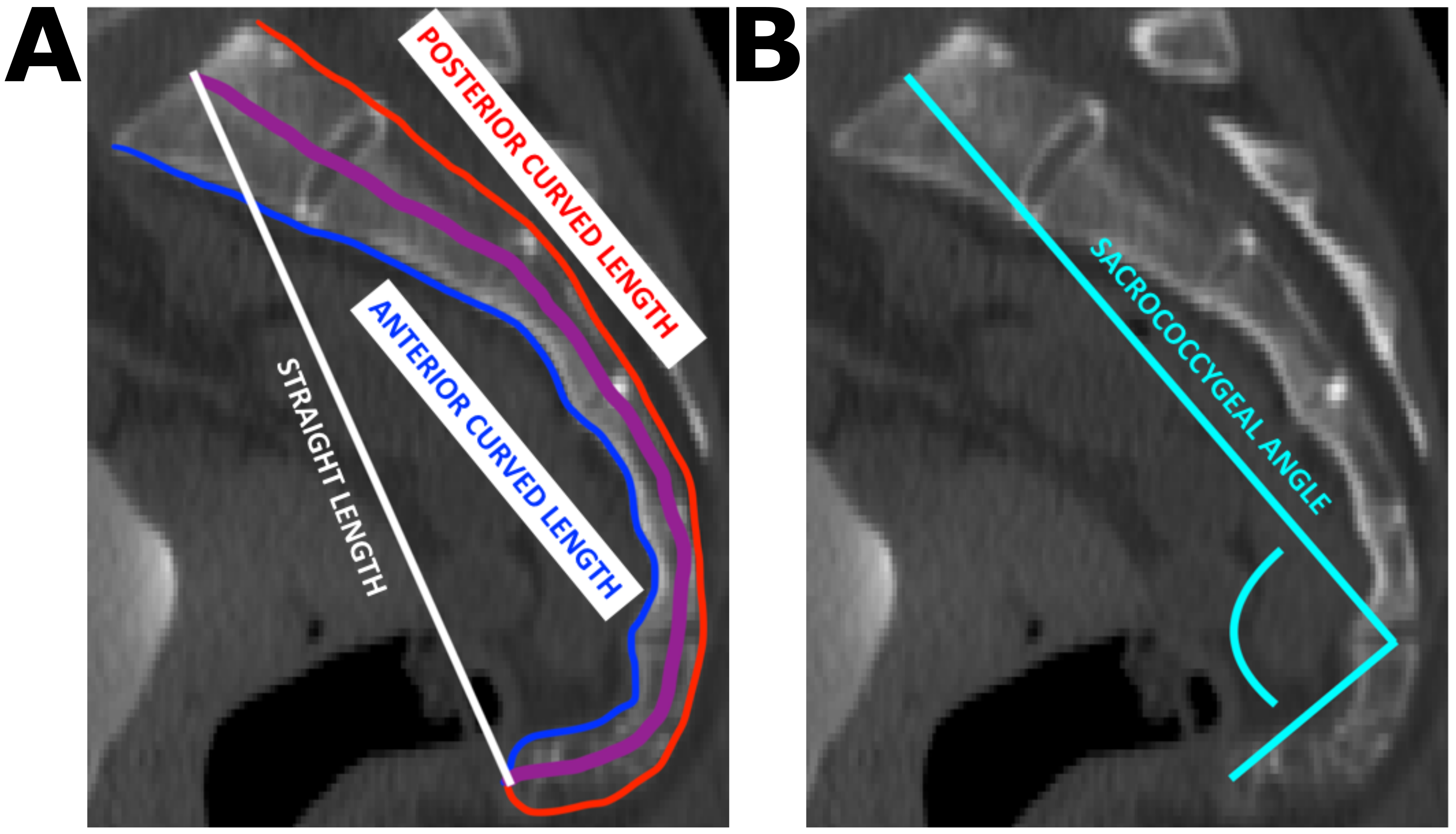
Objective: To identify postoperative vaginal morphology and position factors associated with prolapse recurrence following vaginal surgery. Design: Secondary analysis of MRIs of the Defining Mechanisms of Anterior Vaginal Wall Descent cross-sectional study. Setting: Eight clinical sites in the US Pelvic Floor Disorders Network. Population: Women who underwent vaginal mesh hysteropexy (hysteropexy) with sacrospinous fixation or vaginal hysterectomy with uterosacral ligament suspension (hysterectomy) for symptomatic uterovaginal prolapse between April 2013 and February 2015. Methods: MRIs (rest, strain) obtained 30-42 months after surgery, or earlier for participants with recurrence who desired reoperation prior to 30 months, were analyzed. Prolapse recurrence was defined as prolapse beyond the hymen at strain on MRI. Vaginal segmentations (at rest) were used to create 3D models placed in a morphometry algorithm to quantify and compare vaginal morphology (angulation, dimensions) and position between groups. Main Outcome Measures: Vaginal angulation (upper, lower, and upper-lower vaginal angles in the sagittal and coronal plane), dimensions (length, maximum transverse width, surface area, volume), and position (apex, mid-vagina) at rest. Results: Of the 82 women analyzed, 12/41 (29%) in the hysteropexy group and 22/41 (54%) in the hysterectomy group had prolapse recurrence. After hysteropexy, recurrences had a more laterally deviated upper vagina (p=0.02) at rest than successes. After hysterectomy, recurrences had a more inferiorly (lower) positioned vaginal apex (p=0.01) and mid-vagina (p=0.01) at rest than successes. Conclusions: Vaginal angulation and position were associated with prolapse recurrence and indicative of vaginal support mechanisms related to surgical technique and unaddressed anatomical defects. Future prospective studies in women before and after prolapse surgery may distinguish these two factors. Funding: Eunice Kennedy Shriver National Institute of Child Health and Human Development-sponsored Pelvic Floor Disorders Network (Grant/Award Number: U10 HD054214, U10 HD041267, U10 HD041261, U10 HD069013, U10 HD069025, U10 HD069010, U10 HD069006, U10 HD054215, U01 HD069031); National Institutes of Health Office of Research on Women’s Health; Boston Scientific Corporation; National Academies of Sciences, Engineering, and Medicine’s Ford Foundation Predoctoral Fellowship Program