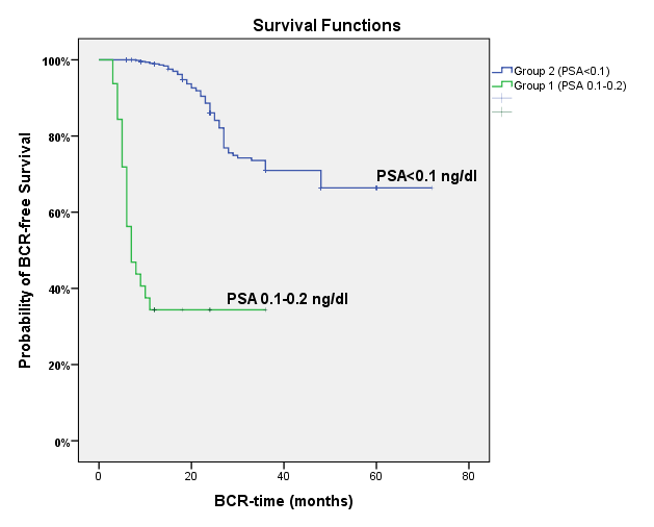
Objective:After radical prostatectomy,prostate-specific antigen(PSA) value measuring ≥0.1ng/ml is defined as persistent PSA(pPSA) and in many studies,it was found to be associated with aggressive disease and poor prognosis.Our aim in this study is to point out the pathological and clinical factors affecting pPSA among the patients who underwent robot-assisted radical prostatectomy(RARP) in an experienced academic center and to make a nomogram,predicting pPSA value based on operative data,useful. Methods:We examined records of 1273 patients who underwent RARP retrospectively. Preoperative,operative,and postoperative data were collected.Based on the PSA values (ng/ml) measured after 4-to-8 weeks of RARP,patients were divided into 2 groups as pPSA group (Group1)(n=97) with PSA values ≥0.1ng/ml and undetectable PSA group (Group2)(n=778) with PSA values <0.1ng/ml.Later on,Group1 was further divided into Group1a (PSA:0.1-0.2ng/ml) and Group 1b (PSA≥0.2ng/ml) to evaluate biochemical recurrence(BCR). Results:Multivariate logistic regression analyses of the collected data revealed that PSA>20ng/ml,operation time,a postoperative international society of urological pathology (ISUP) grade of ≥4, pT 3-4, and pN were independently associated with pPSA.According to the results, a nomogram predicting pPSA was developed(Table 4).By looking at the nomogram pPSA was found in 98.9% of the cases with a PSA value of ≥20ng/ml, an operation time of 150 minutes, a postoperative ISUP grade of 4-5, a positive lymphovascular invasion (LVI) status, pT3-T4, and pN+; while pPSA was found in 25.5% of the cases with a PSA value of <20 ng/ml, an operation time of 100 minutes, a postoperative ISUP grade of <4-5, a negative LVI status, pT<3-4, and pN-.The estimated BCR-free survival time was 16.3 months in Group 1a and 57.0 months in Group2 (p<0.001).Adjuvant treatment ratio was 64.9% in Group1 and 7.1% in Group2 (p<0.001). Conclusion:For the patients who underwent RARP,factors associated with aggressive disease can predict the PSA persistence.To plan our treatment modalities accurately,an applicable nomogram in daily practice would be useful.