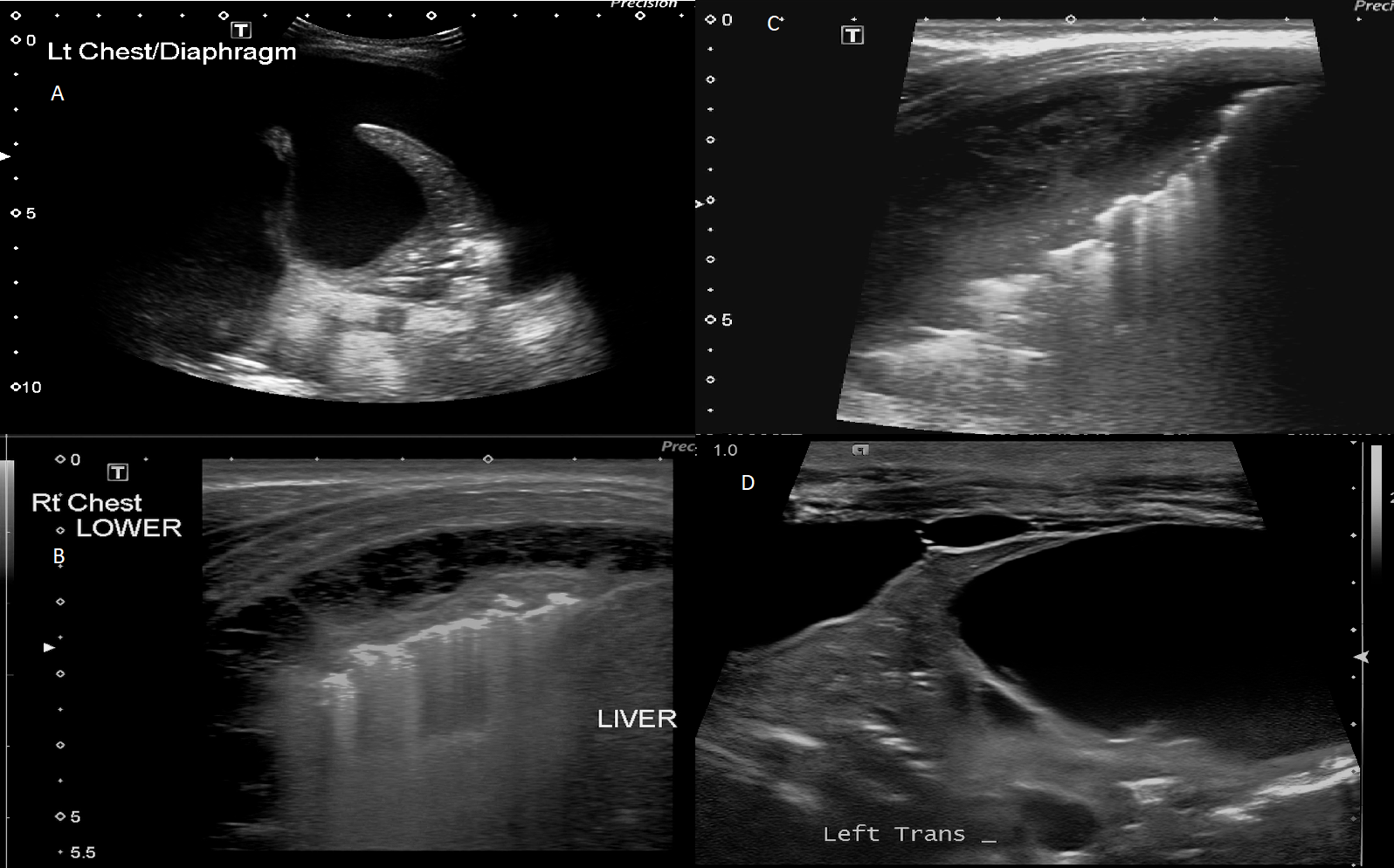
Background: Parapneumonic effusions and empyema are the most frequent complication of paediatric pneumonia. Treatment options include chest drain and fibrinolytics (CDF) or thoracoscopic surgery. CDF is considered less invasive, more cost effective though with higher rates of reintervention. Pleural fluid characteristics on ultrasound may identify cases at increased risk of treatment failure with primary CDF. Methods: A retrospective cohort 2011-2018 of complicated pneumonia managed with primary CDF. Cases were reviewed using ultrasound criteria to describe pleural fluid. We compared ultrasound findings and treatment failure. Results: We report 137 cases with a median age 3.8 years and 43% female. Treatment failure occurred for 32/137 (23%) cases. The interobserver reliability was substantial for the number of septations (Kappa 0.72, 95% CI 0.6 to 0.8), moderate for the size of the largest locule (Kappa 0.55, 95% CI 0.4 to 0.7) and fair for the level of echogenicity (Kappa 0.22, 95%CI 0.1 to 0.3), pleural thickening (Kappa 0.28, 95% CI 0.2 to 0.4), maximum effusion depth (Kappa 0.37, 95%CI 0.2 to 0.5) and radiologist’s risk for reintervention (Kappa 0.32, 95% CI 0.2 to 0.5). Hyperechoic pleural fluid was associated with treatment failure, with cases nearly five times more likely than anechoic fluid to have a reintervention (OR 4.9 95%CI 1.7 to 14.2, p=0.04). Treatment failure was not associated with other variables. Conclusion: We did not find an association between ultrasound characteristics and treatment failure for complicated pneumonia managed with primary CDF. Inter-observer agreement of ultrasound findings was difficult despite more objective criteria.