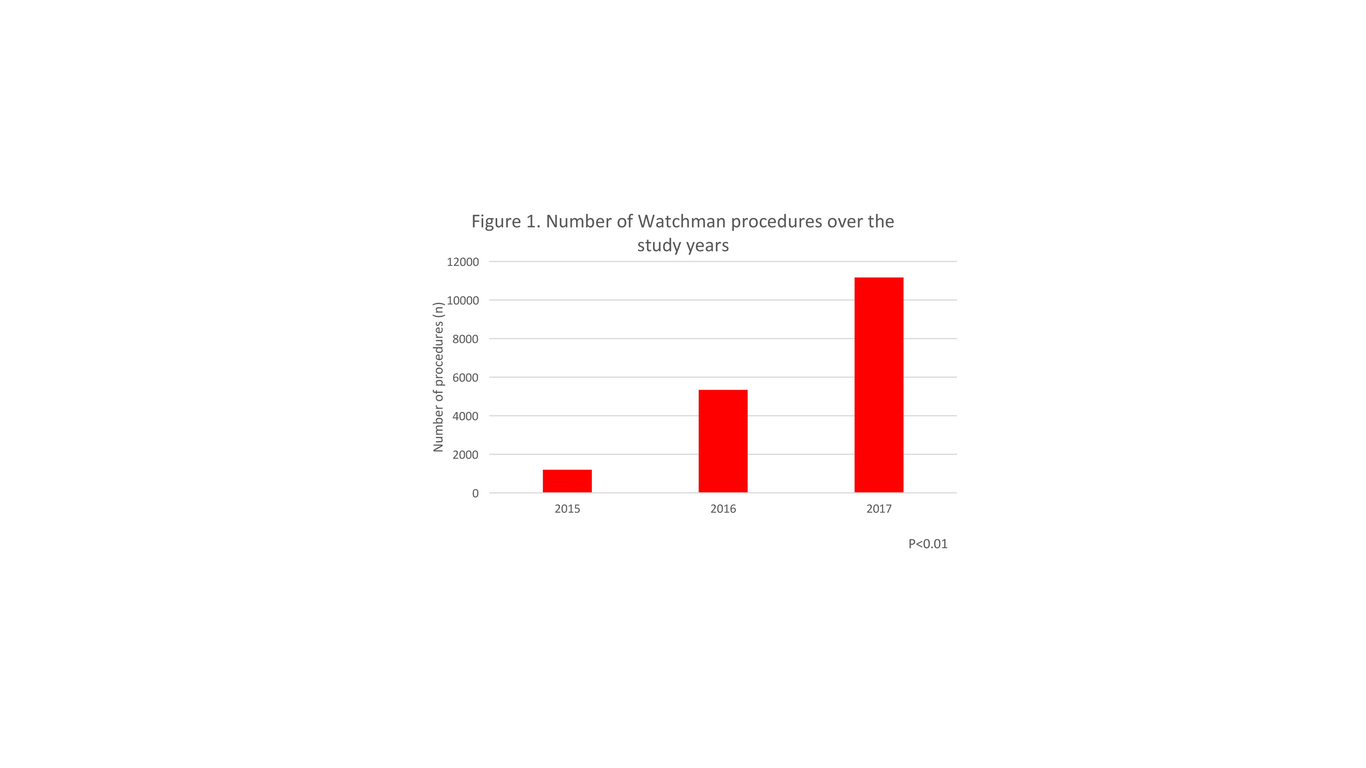
Objective: To determine trends in real-world utilization and in-hospital adverse events from Watchman implantation since its approval by the Food and Drug Administration in 2015. Background: The risk of embolic stroke caused by atrial fibrillation is reduced by oral anticoagulants, but not all patients can tolerate long-term anticoagulation. Left atrial appendage occlusion with the Watchman device has emerged as an alternative therapy. Methods: This was a retrospective cohort study utilizing data from National Inpatient Sample for calendar years 2015-2017. The outcomes assessed in this study were associated complications, in-hospital mortality, and resource utilization trends after Watchman implantation. Trends analysis were performed using analysis of variance. Multivariable adjusted logistic regression analysis was performed to determine predictors of mortality. Results: A total of 17,700 patients underwent Watchman implantation during the study period. There was a significantly increased trend in the number of Watchman procedures performed over the study years (from 1,195 in 2015 to 11,165 devices in 2017, p < 0.01). A significant decline in the rate of complications (from 26.4% in 2015 to 7.9% in 2017, p < 0.01) and inpatient mortality (from 1.3% in 2015 to 0.1% in 2017, p < 0.01) were noted. Predictors of in-hospital mortality included a higher CHA₂DS₂-VASc score (OR 2.61 per 1-point increase, 95% CI 1.91-3.57), chronic blood loss anemia (OR 3.63, 95% CI 1.37-9.61) and coagulopathy (OR 4.90, 95% CI 2.32-10.35). Conclusion: In contemporary United States clinical practice, Watchman utilization has increased significantly since approval in 2015, while complications and in-patient mortality have declined.