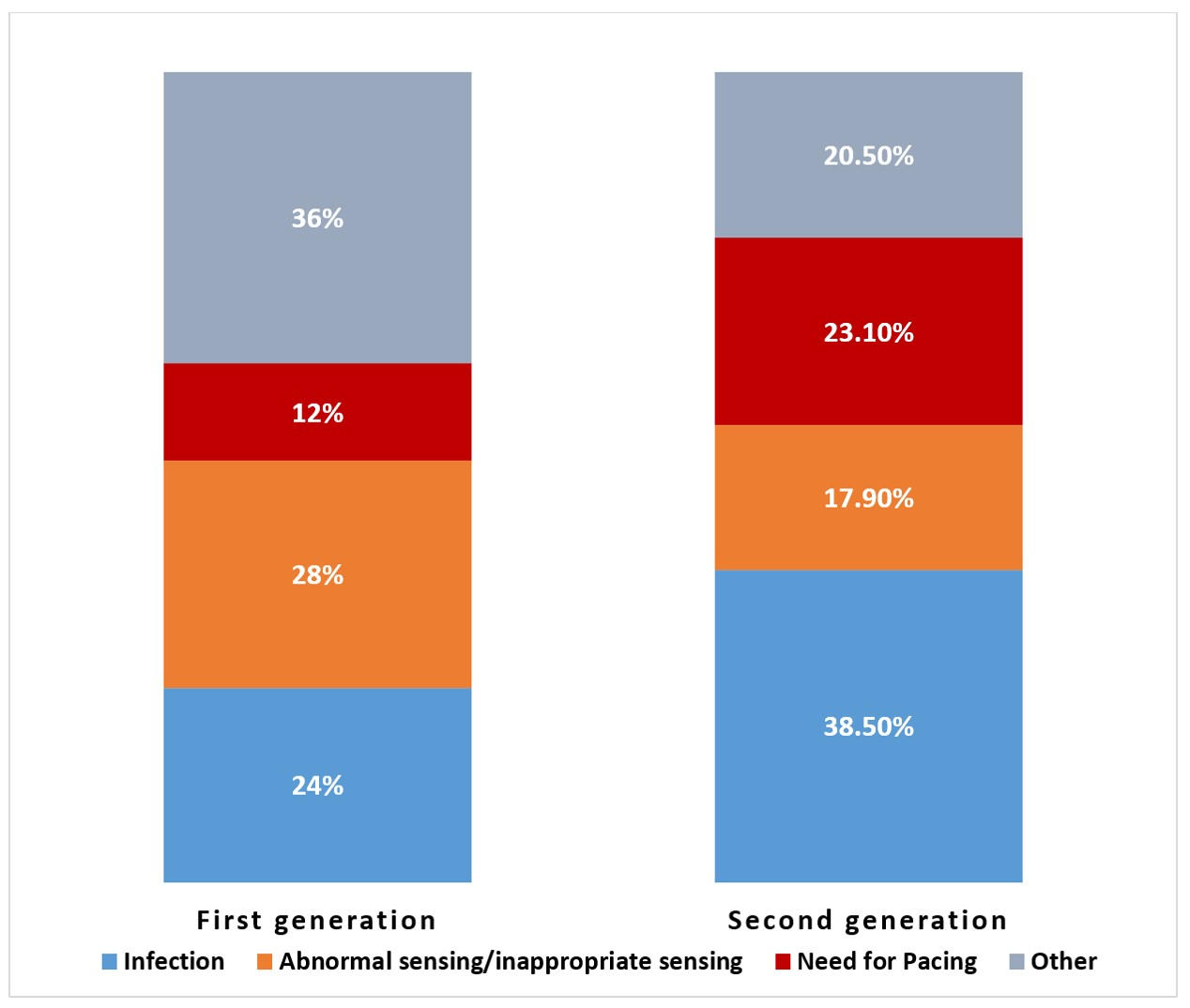
Background: The subcutaneous implantable-cardioverter defibrillator (S-ICD) is an appealing alternative to transvenous ICD systems. However, data on indications for S-ICD explantations are sparse. Objectives: To assess incidence and indications for S-ICD explantation at a large tertiary referral center. Methods: We conducted a retrospective study of all S-ICD explantations performed from 2014 to 2020. Data on demographics, comorbidities, implantation characteristics, and indications for explantation, were collected. Results: A total of 64 patients underwent S-ICD explantation during the study period. During that time, there were 410 S-ICD implantations at our institution of which 53 (12.9%) were explanted with a mean duration from implant to explant of 19.7±20.1 months. The mean age of the patients at explantation was 44.8±15.3 years, and 42% (n=27) were female. The indication for S-ICD implantation was primary prevention in 58% and secondary prevention in 42% of the patients. The most common reason for explantation was infection (32.8%) followed by abnormal sensing (25%) and need for pacing (18.8%). Those who underwent S-ICD explantation for pacing indications were significantly older (55.7±13.6 vs 42.3± 14.6 years, p = 0.005) with a wider QRS duration (111±19 ms vs 98±19 ms, p = 0.03) at device implantation compared to patients who underwent explantation for other indications. Conclusion: Incidence of S-ICD explantation in a large tertiary practice was 12.9%. While infection was the indication for a third of the explantations, a significant number were due to sensing abnormalities and need for pacing. These data may have implications for patient selection for S-ICD implantation.