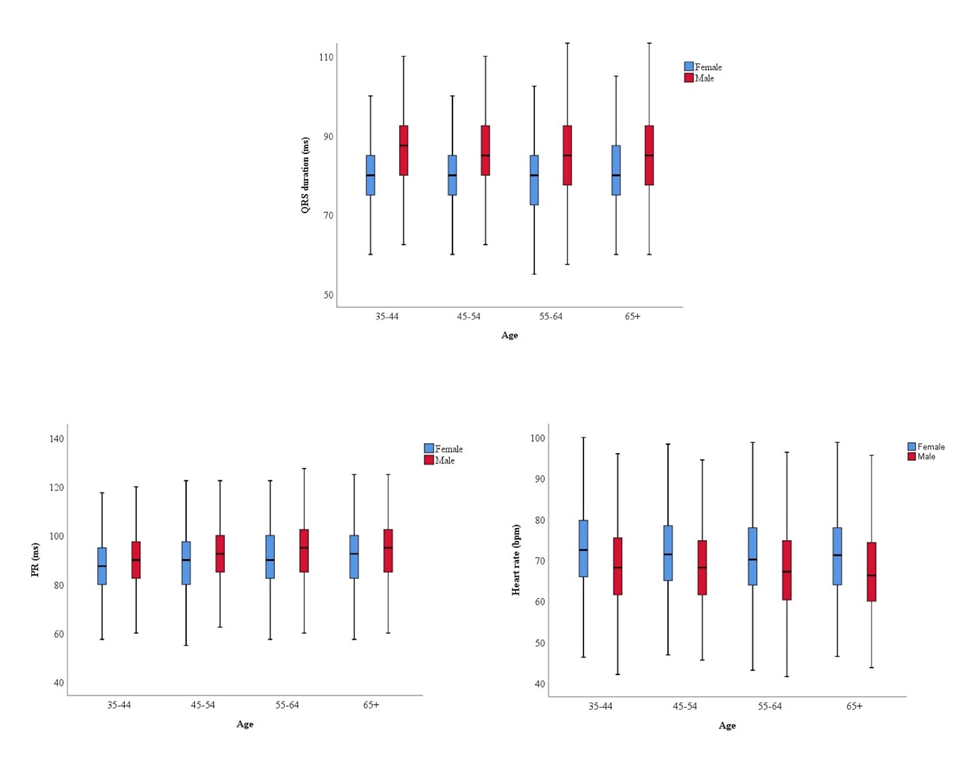
Introduction Although several studies are available regarding baseline Electrocardiographic (ECG) parameters, major and minor ECG abnormalities, there is a big controversy regarding their age and gender differences in literature, thus we aimed to investigate any possible age or gender ECG discrepancies in general adult population. Methods Data of 7630 adults aged ≥35 years from Tehran Cohort Study who were registered between March 2016 to March 2019 were collected. ECG basic values, major, and minor ECG abnormalities-defined according to the Minnesota Code-were analyzed and compared between genders, and four distinct age groups. Odds ratio of having any major ECG abnormality between males, and females stratified by age, and number of cardiovascular risk factors was calculated. Results ECG information of 7630 participants was available. The average age was 53.6 (±12.66), and women made up 54.2% (n=4132) of subjects. The average heart rate (HR) was higher among women(p<0.0001), while the average values of QRS duration, P wave duration, and RR intervals were higher among men(p<0.0001). Major ECG abnormalities were observed in 2.9% of study population (with right bundle branch block, left bundle branch block, and Atrial Fibrillation being the most common) and were more prevalent among men compared to women (3.1% vs 2.7% p=0.188). Moreover, minor abnormalities were observed in 25.9% of study population, and again were more prevalent among men (36.4% vs 17% p<0.001). Prevalence of major ECG abnormalities was significantly higher in participants older than 65 years old, and participants who had ≥3 conventional cardiovascular (CV) risk factors. Conclusion Basic ECG values is different in male and female general population. In addition, major and minor ECG abnormalities were roughly more prevalent in male subjects. In both genders, odds of having major ECG abnormalities surges with increase in number of conventional CV risk factors and age.