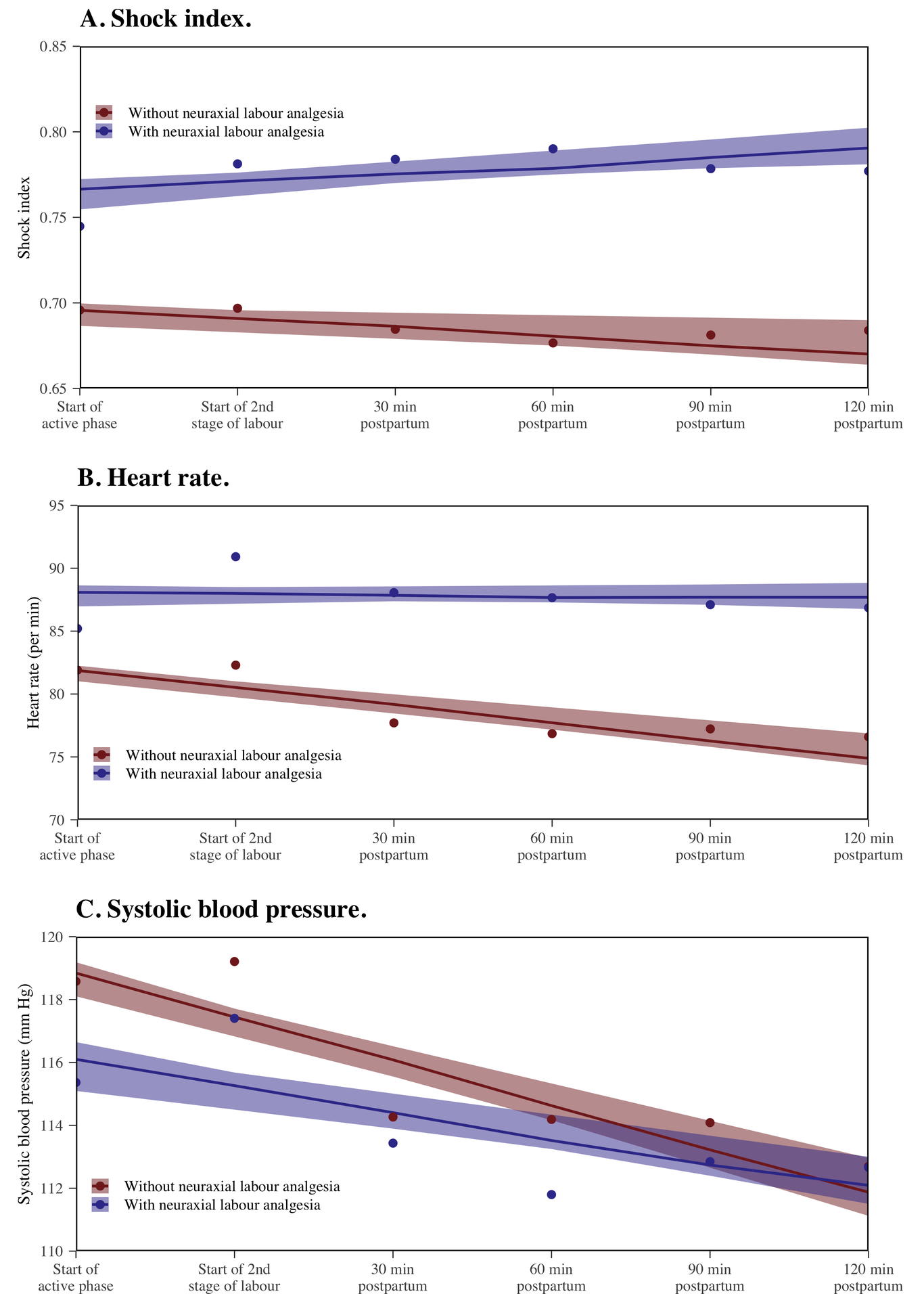
Objective: We aimed to assess the association between intrapartum neuraxial labour analgesia (NLA) and shock index values during the peripartum period. Design: A multicentre prospective cohort study. Setting: Two reference centres in Colombia. Population: Obstetric patients in labour with term gestations were divided according to whether they underwent NLA between 2017 and July 2018. Methods: We collected maternal blood pressure and heart rate within the first and second stages of labour and every 30 minutes up to two hours postpartum. We assessed the association between intrapartum NLA and shock index values in a multivariable longitudinal mixed-effect model, adjusting for covariates. Main outcome measures: Shock index changes over time during labour and postpartum periods. Results: We included 522 patients, 228 (43.7%) with NLA and 294 (56.3%) without NLA. Except in the first stage of labour [0.68 (IQR, 0.63-0.74) vs 0.73 (IQR, 0.64-0.82); p=0.07], the shock index values were significantly higher in patients with NLA during the second stage of labour and postpartum (all p values <0.001). In the longitudinal mixed-effect model analysis, shock index values were higher in the NLA group. After adjusting the multilevel model by age, nulliparity, and cervical dilation, the mean shock index without NLA across the measurements was 0.69, while in NLA was 0.76 (mean difference of 0.067). Conclusions: In patients receiving NLA, the shock index values during labour differ from those during the postpartum period. Thus, under these conditions, the shock index should be interpreted differently. Keywords: Shock Index; Neuraxial Labour Analgesia; Postpartum Haemorrhage.