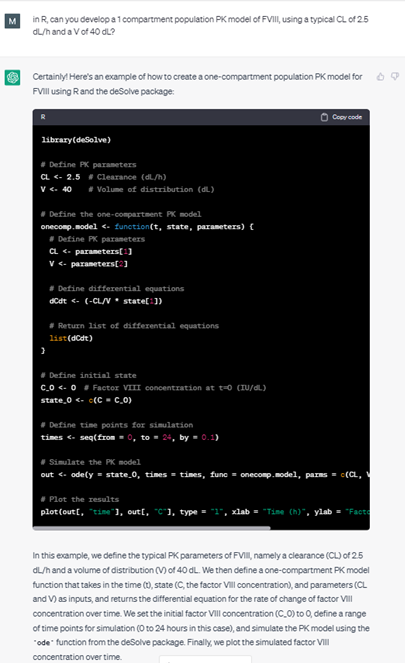
The potential of using chatGPT in pharmacometrics was explored in this study, with a focus on developing a pharmacokinetic (PK) model for standard half-life factor VIII. Our results demonstrated that chatGPT can be utilized to accurately obtain typical PK parameters from literature, generate a population PK model in R, and develop an interactive Shiny application to visualize the results. ChatGPT’s language generation capabilities enabled the development of R codes with minimal programming knowledge and helped identify and fix errors in the code. While chatGPT presents several advantages, such as its ability to streamline the development process, its use in pharmacometrics also has limitations and challenges, including the accuracy and reliability of AI-generated data, the lack of transparency and interpretability of AI. Overall, our study demonstrates the potential of using chatGPT in pharmacometrics, but researchers must carefully evaluate its use for their specific needs.