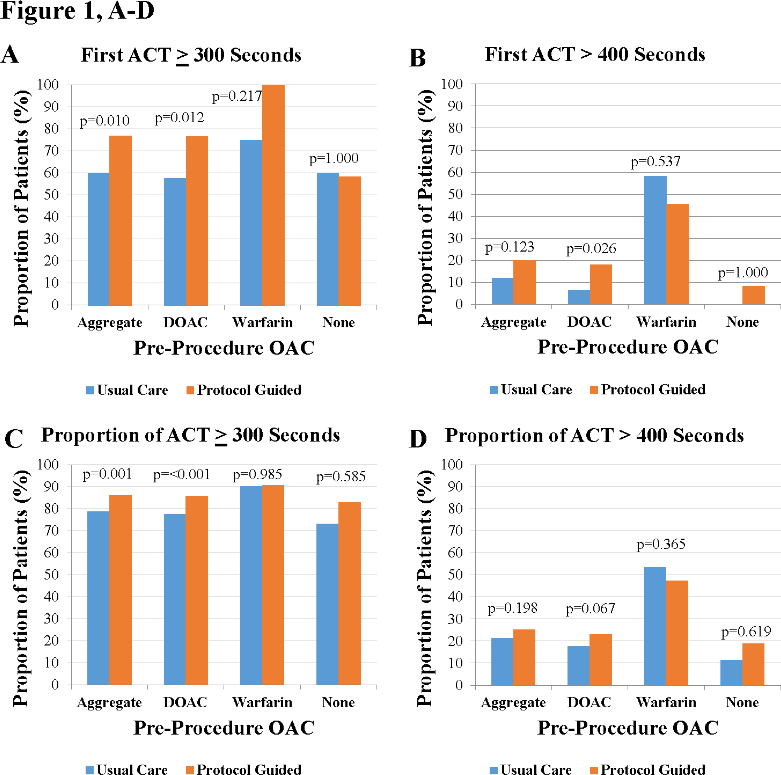
Introduction: A weight-based heparin dosing policy that adjusted for pre-procedural oral anticoagulation was implemented to reduce the likelihood of sub-therapeutic dosing during left atrial catheter ablation procedures. Our hypothesis was that initiation of the protocol would result in a greater prevalence of therapeutic Activated Clotting Time (ACT) values and decreased time to therapeutic ACT during left atrial ablation procedures. Methods: A departmental protocol was initiated for which subjects received intravenous unfractionated heparin (UFH) to achieve and maintain a goal of ACT >300 seconds. Initial bolus dose was adjusted for pre-procedure oral anticoagulation and weight as follows: 50 units/kg for those receiving warfarin, 75 units/kg for those not anticoagulated, and 120 units/kg for those on direct oral anticoagulants. An UFH infusion was initiated at 10% of the bolus per hour. An observational study was performed on 100 consecutive left atrial ablation procedures with usual care, versus 100 with protocol guided peri-procedural care. Results: When usual care and protocol guided cohorts were compared, significant findings were limited to those on pre-procedure direct oral anticoagulant (DOAC). The initial UFH bolus increased from 97±29 units/Kg to 113±29 units/Kg (p<0.001), the proportion of therapeutic ACT on first draw after heparin administration increased from 58% to 77% (p=0.010), and the time to therapeutic ACT after UFH administration decreased from 37.8±19.8 minutes to 30.2±16.4 minutes (p=0.032). Conclusion: A weight-based protocol for peri-procedural UFH administration resulted in a higher proportion of therapeutic ACT values and decreased the time to therapeutic ACT for those on pre-procedure DOAC.