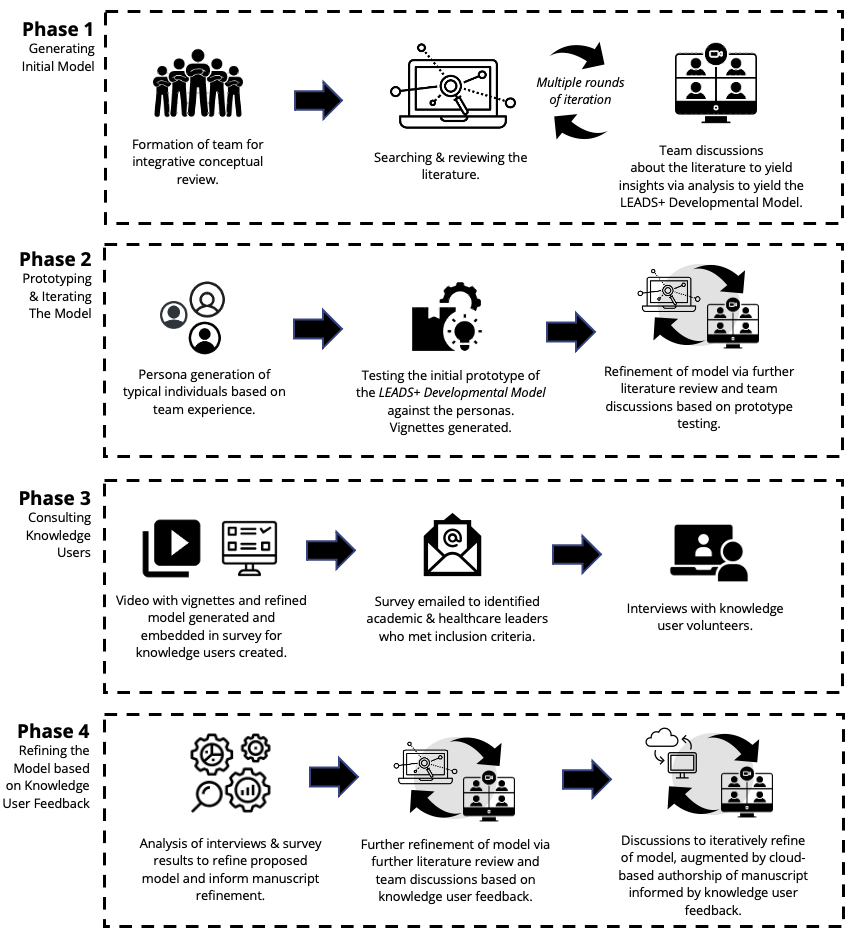
Purpose: Leaders in academic health sciences centres (AHCs) must navigate multiple roles as an inherent component of their positions. Changing accountabilities, varying expectations, differing leadership competencies required of multiple leadership roles can be exacerbated by health system disruption, such as during the COVID-19 pandemic. We need improved models that support leaders in navigating, so they can better handle the complexity of multiple leadership roles.Method: This integrative conceptual review sought to examine leadership and followership constructs and how they intersect with current leadership practices in AHCs. The goal was to develop a refined model of health care leadership development. The authors used iterative cycles of divergent and convergent thinking to explore and synthesize various literature and existing leadership frameworks. The authors used simulated personas and stories to test the model and, finally, the approach sought feedback from knowledge users (including health care leaders, medical educators, and leadership developers) to offer refinements. Results: After five rounds of discussion and reformulation, the authors arrived at a refined model: the LEADS+ Developmental Model. The model describes four nested stages, organizing progressive capabilities, as an individual toggles between followership and leadership. During the consultation stage, feedback from 29 out of 65 recruited knowledge users (44.6% response rate) was acquired. More than a quarter of respondents served as a senior leader in a health care network or national society (27.5%, n=8). Consulted knowledge users were invited to indicate their endorsement for the refined model using a 10-point scale (10=highest level of endorsement). There was a high level of endorsement: 7.93 (SD 1.7) out of 10. Conclusion: The LEADS+ Developmental Model may help foster development of academic health centre leaders. In addition to clarifying the synergistic dynamic between leadership and followership, this model describes the paradigms adopted by leaders within health systems throughout their development journey.